A jaw too wide
Babies opening their mouths too wide may find their jaws dislocated.
Published online 30 November 2015
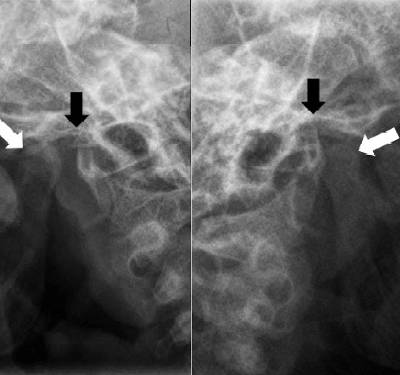
Open mouth view showing condyle (white arrow) and glenoid fossa (black arrow).
© Journal of Emergency Medicine, Trauma & Acute Care
Doctors in Oman report the extremely rare case of a young child whose jaw was dislocated on both sides of her face1.
Writing in the Journal of Emergency Medicine, Trauma & Acute Care, Mohammad Faisal Khilji and Aftab Khalid Malik of Sultan Qaboos University Hospital in Muscat describe a 26-month-old child brought to their emergency department by her mother, who complained that the child had been unable close her mouth, and so could not stop drooling for the last two hours.
Clinical examination of the child revealed no signs of injury, but showed that her lower jaw was displaced forward. As a result of the dislocation, she could not speak or take medicine orally. An X-ray further revealed that both of her temporomandibular joints, which attach the lower jaw to the bottom of the skull, were dislocated.
The doctors sedated the child and manually reduced the dislocations by applying gentle pressure to the lower jaw. About one hour later, she was fully conscious again, and able to close her mouth, speak, and bite properly. She was bandaged to prevent her from opening her jaw too wide, and then discharged.
Temporomandibular dislocation is usually caused by wide mouth opening, traumatic injuries to the jaw, and dental or ear, nose, and throat procedures. It occurs in about 5.3 per 100,000 adult patient, but bilateral dislocations in children such as this are extremely rare, with only three previous case studies in the medical literature. Young women between the age of 21 and 30 are reported to have the highest incidence of the condition.
In the case of this little child, as in the previously documented ones, the woman was instructed to try to prevent her child from opening her jaw widely, for example when yawning or crying, and advised to give he a soft diet that does not require much chewing.
The researchers suggest that doctors in emergency rooms who see cases of children continuously drooling and who fail to close their mouth should consider bilateral temporomandibular joint dislocation and perform reduction quickly, since delays may cause the muscle to spasm more and would then need anaesthesia for reduction.
Reference
- Khilji, M. F. & Malik, A. K. Bilateral temporomandibular joint dislocation in a 26-month-old child: a rare emergency. J. Emergency Med. Trauma Acute Care 2015, 9 (2015). | article
DOI: 10.1038/qsh.2015.88
